 | | | | |  | By Megan R. Wilson | Did someone forward this newsletter to you? Sign up here to get it in your inbox. In today’s issue: How much did your home state receive in health-related congressional earmarks?. … Pharma goes to war with upcoming Super Bowl ads. … The Trump administration proposes new transparency rules for pharmacy benefit managers. Happy Friday, and welcome back to Health Brief. It looks like there’s been an agreement in the Senate to vote on five of the government funding bills — including the one with money for major health agencies — and a stopgap measure to temporarily fund the homeland security agency while lawmakers hammer out some reforms. → If the White House-endorsed compromise passes the Senate, the House could vote as soon as Monday. This means there will be a (very brief) partial shutdown, as funding expires on Saturday. It’s Feedback Friday. What’s on your mind? Don’t forget to send story tips and health policy intel to megan.wilson@washpost.com. If you prefer to message me securely, I’m also on Signal at megan.434. This newsletter is published by WP Intelligence, The Washington Post’s subscription service for professionals that provides business, policy and thought leaders with actionable insights. WP Intelligence operates independently from the Washington Post newsroom. Learn more about WP Intelligence. | | | |  | The Lead Brief | Senators are directing nearly $1 billion in federal cash to health care-related initiatives in their own states, including for purchasing new ambulances, buying equipment to expand access to telehealth and funding investments in workforce development and mental and behavioral health programs. I crunched the data for all the earmarks included in the Labor-HHS appropriations bill, which includes funding for the Department of Health and Human Services, the Department of Labor and the Department of Education. The data includes all earmarked funds at HHS agencies and the health-related projects at the Labor and Education departments. (The House does not allow earmarks on the Labor-HHS bill.) → Overall, it’s a fraction of the $16 billion in earmarks the entire government funding package contains, according to a tally from Politico. | 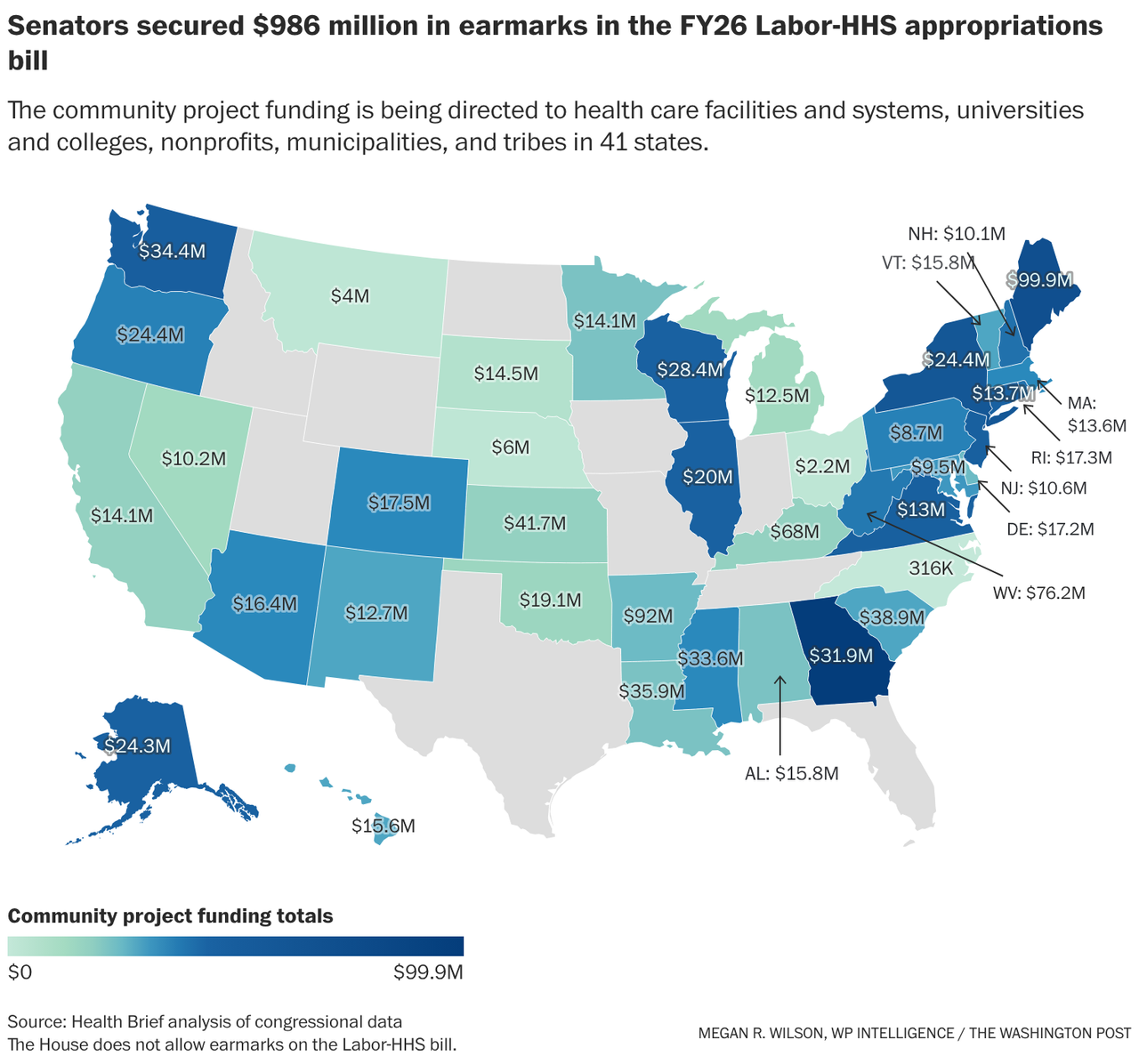 | | Overall, here are the key figures within the $986 million: The top recipients of health earmarks are, unsurprisingly, members of the Senate Appropriations Committee. Proponents of earmarks argue that they’re a way for Congress to exert control over where federal money goes rather than allowing the executive branch to decide. - Sen. Susan Collins (R-Maine), who leads the appropriations panel, brought home the most money to her state in the Labor-HHS bill: $97.5 million, including the $38.7 million in projects she requested with Sen. Angus King (I-Maine).
The money went to 33 projects, including $10.8 million to MaineHealth Stephens Hospital to expand its emergency department and oncology infusion center, millions of dollars in support for various health workforce training programs, and more than $1.9 million for the MDI Biological Laboratory to support construction of the Center for Advancing Science Education and Entrepreneurship on its Bar Harbor campus. Individually, King secured $2.3 million to help Community Dental, a Maine nonprofit, expand its dental services. That brings Maine’s overall health project funding in the appropriations bill to $99.9 million — the most of any state. - The University of Arkansas for Medical Sciences was the single-largest recipient of earmarked health care funds. Sen. John Boozman (R-Arkansas) earmarked $40 million for seven different projects at the university, including a $15 million line item to expand and renovate its labor and delivery unit.
The University of Arkansas for Medical Sciences is “the state’s only academic health center, hence the substantial support for its programs and initiatives,” Boozman’s office tells me in an email. Boozman, who sits on the appropriations panel, secured $92 million for entities in his state overall. Other large projects include a $15 million project to construct the a center focused on maternal and infant health at the University of Arkansas-Fort Smith and $13.3 million to help the Arkansas Department of Health upgrade its technology, including its electronic medical records system and purchasing telehealth equipment and remote patient-monitoring tools. “The senator put an emphasis on improving health outcomes,” Boozman’s office said, “and looks forward to these projects being implemented to enhance the services providers and institutions deliver for Arkansans.” - Sen. Jon Ossoff (D-Georgia) helped fund the largest number of health care-related projects (40), including the 13 he co-requested with Sen. Raphael G. Warnock (D-Georgia).
Ossoff, another member of the appropriations panel, is up for reelection this year, and will be able to point to several projects benefiting the state: $2 million to help expand Georgia’s 211 system, which connects residents to local health and human services, nearly $500,000 to support two diaper distribution programs for low-income families, and $357,000 toward an opioid overdose prevention program. Overall, Georgia will be receiving $31.9 million in earmarked funds for 46 individual health initiatives. - Senators have allocated cash for a total of 602 health-related projects. Republicans received more money for health care earmarks ($540.9 million) than Democrats ($404.6 million), but Democrats funded a larger number of projects (423) than Republicans (161). There was also $40.4 million worth of jointly requested bipartisan health earmarks, funding 18 different projects.
| | | | | | Numbers Game | Here are some other spending trends: - More than one-third of all health-related earmarks ($313.8 million) went to construction and renovation projects, including to build new hospitals, expand education, workforce training and research facilities at colleges and universities, an operating room, health clinics, and behavioral and substance use disorder treatment centers.
- More than $68 million is going to various technological upgrades at health facilities, colleges and universities, including $15 million to the Charleston Area Medical Center to upgrade its cybersecurity and technological infrastructure, as requested by West Virginia Republican Sens. Shelley Moore Capito and Jim Justice. (West Virginia secured a hefty $76.2 million in health project funding overall.)
- Senators allocated $34.6 million to fund mobile health clinics or units, including vision and dental clinics, mobile mental health and substance use disorder treatment units, and mobile clinics to provide pediatric care. Another $13.5 million went to purchase new ambulances or expand ambulatory services.
On Friday, the Senate blocked an amendment by Sen. Mike Lee (R-Utah) to strip all earmarks from the funding package in a 63-33 vote. Rep. Ralph Norman (R-South Carolina) had also attempted to strip the Senate’s earmarks from the Labor-HHS bill, saying that the project funding “undermines trust and invites waste.” “Federal funding should prioritize working families, public health, and responsible governance. Not partisan pet projects,” he said in a statement touting support from conservative groups Heritage Action and the Club for Growth. |  | | The battle over GLP-1 medication market share will play out during the Super Bowl. (JoNel Aleccia/AP) | | | | | | Industry Rx | The Super Bowl will feature more than just a battle of two football teams, as pharmaceutical manufacturers and telehealth companies both fight for Americans’ attention — and dollars. Hims & Hers will present an ad touting its telehealth services and access to diagnostic testing, hormone treatments, and compounded GLP-1 medications, the cheaper copycat versions of the weight loss drugs that have drawn ire from the pharmaceutical companies. The minute-long spot argues the platform gives regular consumers access to the personalized type of care that wealthy individuals have. “Rich people live longer,” says a voice-over by rapper and actor Common in the ad. “The wealth gap is a health gap.” Why it matters: The Super Bowl drew more than 120 million viewers last year, providing companies with a massive audience to sell their wares. Deciding to wade into the Super Bowl advertising illustrates how important the fight over market share is for these companies — because it ain’t cheap: A 30-second spot during the Super Bowl sets companies back about $10 million, according to Bloomberg. Meanwhile, drugmakers Eli Lilly, which makes Zepbound, and Wegovy-maker Novo Nordisk will also be airing their own spots. Novo Nordisk has been teasing an unaired spot, with multiple celebrities, including SNL’s Kenan Thompson and rapper DJ Khaled, posting about it on social media. Eli Lilly is planning an advertising campaign around Zepbound, including a pregame advertisement that will air “simultaneously across NBC, Peacock and Telemundo, followed by an in-game [ad] airing exclusively on Peacock,” the company confirmed. Another telehealth platform, Ro, has enlisted Serena Williams for its own ad that will air during the Feb. 8 matchup that promotes her experience with GLP-1 weight loss drugs. The endorsement from Williams has translated into serious sales, with Ro saying that it received a sustained spike in new customers after it began partnering with the tennis legend last August. Washington will be watching: Federal regulators dinged Hims & Hers for its Super Bowl ad that featured GLP-1 products last year, with Food and Drug Administration Commissioner Marty Makary arguing that the ad highlighted the benefits of the drugs “without any mention of side effects or disclaimers.” | | | | | | Executive Health Brief | The Department of Labor on Thursday announced a proposal to require intermediaries known as pharmacy benefit managers, or PBMs, to be more transparent with certain employer-sponsored plans about their fees, compensation and rebates from drugmakers. PBMs negotiate discounts on medications with drugmakers, and then decide which drugs insurance plans will cover. Critics have argued that the industry’s largest players have outsize influence on rising drug costs, while PBMs say they work to cut deals with pharmaceutical companies to keep costs down. With this proposal, Labor Secretary Lori Chavez-DeRemer said in a statement that the department is “delivering unprecedented transparency to an otherwise opaque industry.” Under the proposal, PBMs would have to disclose: - The money they receive when a health insurance plan pays more for a prescription medication than a pharmacy is reimbursed by PBMs for dispensing it, a practice known as “spread pricing” that has drawn criticism from policymakers.
- Information about the rebates PBMs receive from drugmakers and “any formulary placement incentives” they take while determining which medications a health plan will cover.
- Details about the money they receive from pharmacies “in connection with prescription drugs dispensed to the plan.”
→ The proposal allows a PBM’s employer clients to audit the disclosures for accuracy. “When middlemen are forced to operate in the sunlight, American workers and their families win,” Chavez-DeRemer said. “Hidden fees and distorted incentives have no place in American healthcare.” What it doesn’t do: The proposal is focused on transparency, so it doesn’t ban some of the business practices — such as spread pricing — that lawmakers have sought to limit. The administration estimates that 9.5 million Americans would benefit from the proposed rules, in part because they would apply only to health plans in which employers assume all financial risk for an employee’s medical claims, a small fraction of the market. Roughly 165 million people have insurance through their own or a family member’s employer. → The industry argues that it has already been making moves to be more transparent with plan sponsors. “We appreciate the desire to bring greater transparency across the drug supply chain, which is why PBMs have significantly reformed their models to maximize transparency in recent years,” said Greg Lopes, a spokesperson for the Pharmaceutical Care Management Association, a PBM industry group. “PBMs continue to create new models to offer employers contractual options that meet their expectations to lower costs transparently.” Comments on the proposed rule are due by March 31. The proposal, which stems from one of President Donald Trump’s executive orders on drug pricing, is aligned with some of the provisions targeting PBMs in the government funding bill. - One of those provisions would require PBMs to “pass through” any rebates on medications that they receive from drugmakers to the commercial health plans with which they contract.
- There are also transparency provisions in the measure that require PBMs to disclose information about drug spending and spread pricing arrangements.
Cynthia Fisher, founder and chair of PatientRightsAdvocate.org, argues that the “sunlight on prices and fees” provided by the proposal “will eliminate the nonvalue, middlemen overreach, and will hold billing and payments accountable.” “We urge the Trump administration to go even further and require full transparency for all middlemen and the entire health plan, which would reveal spread pricing and empower employers and unions to redirect savings toward wage growth and corporate earnings,” Fisher said. | | | | |
_tstmp_1756933376-1920-1080.png)


